 Lipoatrophia
Semicircularis:
Lipoatrophia
Semicircularis:
a new office disease?
900 cases reported in Belgium
Click here for word document
Lipoatrophia
Semicircularis: a new office disease?
Curvers
Bart *, M D, occupational physician; Maes Annemarie **, Ph D, senior researcher
Short running title: Lipoatrophia Semicircularis
* KBC Bank & Insurance
Group, Medical Services, Havenlaan 2, B-1080 Brussels Belgium
** VITO (Flemish
Institute for Technological Research), Expertise Center of Environmental Toxicology,
Boeretang 200, B- 2400 Mol, Belgium
Corresponding
author:
Bart L. Curvers
KBC Bank & Insurance Group
Medical
Services
Havenlaan 2
B- 1080 Brussels
Belgium
Phone:
+ 32 2 429 85 00
Fax: + 32 2 429 81 50
Email: bart.curvers@kbc.be
Abstract
The medical literature describes lipoatrophia semicircularis as a rare,
idiopathic condition, that consists clinically of a semicircular zone of atrophy
of the subcutaneous fatty tissue located mostly on the front of the thighs. The
disorder is mainly afflicting office workers. Since 1995, we have diagnosed more
than 900 cases in our company. Also in other companies (national and international)
lipoatrophia semicircularis is diagnosed.
Several hypothesis were proposed,
but no one could explain the symptoms. Although the exact cause is still unknown,
we believe that electromagnetic fields play an important role in this phenomenon.
Introduction
Lipoatrophia
semicircularis (LS) consists clinically of a semicircular zone of atrophy of the
subcutaneous fatty tissue located mostly on the legs. Skin and underlying muscles
remains intact. It is important to distinguish between the annular form of lipoatrophia
and the acquired forms which develop as a consequence of injections.(1,2)
The
phenomenon was reported for the first time in three patients in 1974 by Gschwandtner
and Munzberger.(3,4) Since then, there have been some publications, but these
relate only to 70-odd patients, whereas in our bank and insurance group we have
had several hundreds cases.
Till
now the aethiology of LS is unknown, the literature is mainly descriptive and
as regards aetiology very hypothetical. The cause of LS remains so far speculative,
most authors invariably hypothesize local mechanical pressure (microtraumata caused
by either repetitive pressure against an object or by wearing tight clothing)
as being on its origin.(3-12)
Clinical
observations and pathology
Our
story is a remarkable one. In the Spring of 1995, a total of 1100 -bank employees
moved to our new office building in Brussels. The building was equipped with new
data cabling, new furniture and new telephones, though most of the computer equipment
was the same equipment used in our previous premises. In June 1995, a number of
women were diagnosed with lipoatrophia semicircularis (LS) for the first time.
Six months later, as many as 135 persons had developed this disorder and at the
time of writing, nearly 8 years on, we have registrated more than 900 cases. In
our local branches and other companies, too, there are increasingly more incidences
of this problem. Also in other countries (e.g. France, Italy, U.K. and the Netherlands)
LS is diagnosed.(16 - 20)
The disorder is mainly and mostly exclusively
afflicting administrative (computer working) people.
Typically, the
lipoatrophic zone is localized on the anterolateral side of the thigh,
72 cm above the floor (data gathered on patients wearing shoes) -
72 cm is also the standard height of our office furniture. The lesion
can be uni- or bilateral and is between 5 and 20 cm long, about 2
cm wide and 1 to 5 mm deep. The skin remains intact.(fig. 1,2,3) By
the onset of the lesions (mostly 2 or 3 months after moving into a
new office), some patients mentioned a feeling of heaviness, some
experienced a tingling or burning sensation, while others suffered
from an increased degree of fatigue.
The lesions could disappear spontaneously after several months, but mostly
improved only when people moved to another location in the building, were absent
from work for a long time or were on maternity leave. However, the atrophy would
come back when they returned to work in the same environment.
LS seems
to be reversible. 95% of the retired employees, have no more lesions one year
after leaving the company.
In
anatomopathological research a perivascular lymphocytic infiltration is observed
in the initial phase. In the next phase, there is a decrease in both the volume
and number of adipocytes and after that a gradual replacement of the adipocytes
by connective tissue. The adipocytes are reabsorbed by lysosomally active macrophages.(18
-19, 21 - 22) It is not clear whether the macrophages are the cause (by producing
cytokines) or the consequence of cell destruction.
Echography,
MRI or EMG research did not reveal any other abnormalities.
Personal
data were recorded and from these it emerged that 84% of the disorders occurred
in women, that the pathology was distributed over age groups in accordance with
the employees' age pyramid and that there was no link with any other medical disorder
among the employees affected.
Discussion
So far, the aethiology of lipoatrophia semicircularis is not known.
The literature is mainly descriptive and very hypothetical as regards aethiology.
LS must be due to a new additional factor to which people are exposed in their
working environment.The lesions mostly appeared within 2 or 3 moths after moving
to a new working environment.
Several
authors go no further than microtraumata caused by either repetitive
pressure against one object or another or by tight clothing.(9 - 12) However,
this reason is too simple to explain the problem we have experienced since 1995.
Firstly, if local pressure is the cause of lipoatrophia, it is amazing that we
have had to wait until now to see this pathology. Secondly, local pressure can
cause a local impression, but this will always disappear minutes or hours after
exposure and has no relation to atrophia of the fatty tissue.
Explanations
have also been sought in the area of blood circulation.
The
hypothesis of an anatomical variant has been proposed in which the A.circumflexa
femoris lateralis originates on the A. femoralis and not on the A. profunda femoralis.(
9) As a result, the A. circumflexa femoris lateralis is more distally
located, so that pressure is exerted on this artery when a person sits down, giving
rise to an ischaemic atrophy on the front of the thigh. From a purely anatomical
point of view, pressure on a small part of the thigh seems to be a barely credible
explanation, but most significantly this anatomical variant is found to exist
in only about 3% of the population. This theory is therefore untenable when account
is taken of the large size of our patient group.In one of our buildings, more
than 30% of the employees was affected!
Using the same
line of reasoning, it has been expounded that excessively intense
muscular activity when swivelling around in
an office chair could result in ischaemia in the subcutis. EMG research
(see above) has revealed that a floor covered in linoleum required
far less muscular strength to move about on than was the case with
a carpeted floor. With carpeting, up to 80% of the maximum muscular
strength of the M. Quadriceps and 50% of the strength of the hamstrings
is used; with linoleum these values are one-third lower. Therefore,
it was decided to conduct an experiment by replacing wall-to-wall
carpeting with linoleum. This operation did not yield any clinical
results.
Because
the sitting posture and particular characteristics of the chair
could have an influence on the compression pressure on the distal
side of the back of the thigh and therefore might cause a vascular disturbance,
an ergonomic investigation focusing on the sitting position was carried out by
the University of Louvain.(13) The tables and chairs complied with ergonomic guidelines,
but on the whole the staff were seen to sit fairly high and not to make use of
the arm- and back rests, even though the chair was equipped with these features.
In an analysis of body posture (the aim of which was to avoid musculoskeletal
complaints), it was established that more than half of the employees did not make
use of the lumbar backrest, bent the head far forward when working and assumed
a fairly static body posture; just under half of the workers did not use any rest
for the forearms.
Further investigations were carried out on 21 workers
(11 with and 10 without LS).(13) A video analysis was made of postures and movements
and an electromyographic measurement was made in order to study the muscular tension
on the front and the back of the thigh. In addition, a technological study of
the pressure conditions below the thighs was carried out by using a 42x42 cm pressure
pad which contained a grid of 512 capacitive sensors. From the video recordings
and the electromyographic observations it clearly emerged that persons with Ls
moved less, sat further forward on the chair and had a tendency to sit too high.
The pressure measurements demonstrated that pressure increased by more than 30%
at the distal extremity of the thigh when the seat of the chair was 5 cm too high
in relation to the ideal height and that a footrest was a very good way of addressing
this problem. When the seat is tilted forward (i.e. an open angle), pressure is
at its lowest. However, the research demonstrated that there was no difference
between those who suffered from lipoatrophia and those who did not.
It
was decided to remedy this by offering those who were interested an individual
assessment of their own sitting posture. 176 employees were surveyed, which led
to an improvement of the posture at work and a decrease in musculoskeletal complaints
in a number of staff members, but did not bring about any improvement of the phenomenon
of LS.
Recently,
a new study on sitting was carried out. The hypothesis was that a bad sitting
posture causes shearing forces on the back of the thigh, which can cause an ischeamic
zone on the front side of the leg, thus leading to lipoatrophia. This study was
carried out with the University of Rotterdam (Nl), but failed to come up with
a solution to our problem.(14)
In our situation, the following question arises: what has changed
in the work situation as a result of the move to the new premises?
The more obvious new factors were the building, furniture and wiring.
A large-scale technical research project was carried out.
A specialized firm of consultants conducted an investigation into indoor
air quality: The degree of dust creation was considered to be good or
very good everywhere; the CO2 content was not above 600 ppm anywhere; the microbiological
quality was good, including the concentrations of endotoxins. Thermal comfort
was good, but the relative humidity was too low (around 40%). The ozone content
in the surrounding air never reached 0.01 ppm and the radon content above ground
remained under 20 Bq/m³ and below ground 40-70 Bq/m³, where the limit
value in dwellings is 150 Bq/m³. Radioactivity in the building did not exceed
the measurements for the surrounding environment.
A pilot study for electric
and magnetic fields was carried out, first at the frequency of 50 Hz.(15)
The magnetic field fluctuated for the most part around 0.2 mG, with an occasional
value of 2 mG, the recommended maximum. The electric field ranged up to 150 V/m
for a non-earthed cable conduit full of cables; when the cable conduit was earthed,
the value never exceeded the standard value of 16 V/m. The electric field strengths
were always appreciably higher when someone was seated at the workstation than
when not. From the findings of this research, a proposal was made to earth all
workstations. The clinical results of this earthing have been conspicuous by their
absence.
A subsequent study included the VLF and LF fields, as well as
the ULF or microwave frequencies at 915 and 2450 MHz. No abnormally high magnetic
field strengths were observed anywhere, compared with the generally accepted underground
load or limit values.
Another hypothesis related to electrostatical
discharge (ESD) to the thighs via the desk top.(26 - 27) In this hypothesis,
the conductivity of the desk top plays a mayor role; the surface resistance varies
from 20x10 to 1x10.ohms according to the material and finish of the desk tops
examined. Preferably, they should be as low as possible.
Local electrostatic
discharges on that region of the legs, where the human body is coupled with the
edge of the table, can in a biological plausible way explain what is happening
in the lipoatrophic tissue. Activated macrophages produce cytokines; e.g. TNFa
that is able to damage adipocytes and modify the structure of adipose tissue.(22
- 25)( fig.4) Extensive experiments have been carried out with ALU plate and ALU
post in which data and other cables are stored, but all experiments failed to
produce any noteworthy results.
A new pilot project in the electromagnetic
domain was recently completed. The goal was to limit the amount of litter
on the cable network. To this end, the entire cabling (for the PC network, telephones
and electricity) on one floor was replaced with ferrite cables. This has drastically
reduced the litter and the electromagnetic fields it creates. There has been a
clear improvement in the condition of those employees affected by LS. In some
cases there has been a complete recovery. To-date, this is the only trial
to have given a positive result for all those affected. This reinforces
our belief that the cause of LS should be sought in the area of electromagnetics.
(27)
Conclusion
This
report sets out the history of a remarkable problem, a problem we are still trying
to find a solution to. Although this disease is catalogued as a very rare one,
it is now occurring very frequently at least in certain workplaces.
We
may concluded that the frequent occurrence of lipoatrophia semicircularis is directly
related to modern new office buildings and new working environments. Probably
the cause as well as the solution is a multifactorial one. Although the cause
is still unknown, we believe that electromagnetic fields play an important role
in this phenomenon.

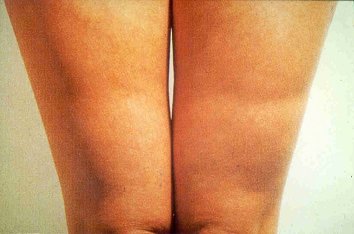
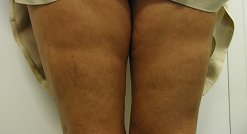
Fig. 1,2 and 3 : Semicircular zones of lipoatrophia on the
front of the
thighs
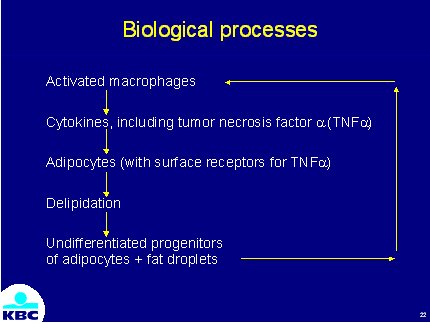
Fig. 4 : Biological
hypothesis of the atrophia of the subcutaneous fatty tissue.
REFERENCES
1. Atlan-Gepner C, Bongrand P, Farnarier C, Xerri L, Choux R, Gauthier J.F,Brue
T,Vague P, Grob JJ, Vialettes B. Insulin-induced lipoatrophy in type I diabetes.Diabetes
Care.1996; 9: 1283-1285.
2. Imamura S, Taniguchi S. Lipoatrophic lesions
preceded by pain and erythema a new clinical entity? Eur. J. Dermatol. 2000; 10:
540-541
3. Gschwandtner
WR, Münzberger H. Lipoatrophia semicircularis. Ein Beitrag zu bandförmig-circulären
Atrophien des subcutanen Fettgewebes im Extremitätenbereich. Der Hautartz
1974; 25: 222-227
4.
Gschwandtner WR, Münzberger H. Lipoatrophia semicircularis. Wiener klein.
Wochenschr. 1975; 87: 164-168.
5.
Karavitsas C, Miller JA, Kirby JD. Semicircular lipoatrophy. Brit. J. Dermatolol.
1981; 105: 591-593.
6.
Ayale F, Lembo G, Ruggiero F, Balato N; Lipoatrophia semicircularis,report of
a case. Dermatologica 1985; 170:101-103.
7.
De Rie MA. Indrukken op de bovenbenen ; Lipoatrophia semicircularis. Ned. Tijdschr.
Geneesk. 1998; 142: 796-797.
8.
Nagore E, Sanchez-Motilla JM, Rodriguez-Serna M, Vilata JJ, Aliaga A. Lipoatrophia
semicircularis- a traumatic panniculitis : report of seven cases and review of
the literature. J. Am. Acad. Dermatol. 1998; 39: 879-881.
9.
Bloch PH, Runne U. Lipoatrophia semicircularis bein Mann. Zusammentreffen von
Arterienvarietaät und Microtraumata als mögliche Krankheitsursache.
Der Hautartz 1978; 29: 270-277.
10.
Mascaro JM, Ferrando J. The perils of wearing jeans: Lipoatrophia semicircularis.
Int. J. Dermatol. 1983; 22: 333.
11.
Hodak E, David M, Sandbank M. Semicircular lipoatrophy - a pressure-induced lipoatrophy?
Clin. Exp. Dermatol. 1990; 15: 464-465.
12.
De Groot AC. Is lipoatrophia semicircularis induced by pressure? Brit. J. Dermatol.
1994; 131: 887-890.
13.
Hermans V, Hautekiet M, Haex B, Spaepen AJ, Van der Perre G. Lipoatrophia semicircularis
and the relation with office work. Appl. Ergonomics 1999; 30: 319-324.
14.
Verbelen C. Lipoatrophia semicircularis in relatie met zitten vanuit het biomechanisch
model. BMA Ergonomics 2002.
15.
Decat G. Evaluatie van de elektromagnetische velden in de werkomgeving van het
hoofd- en enkele bijkantoren van de Kredietbank. Vito report 1997; TAP.RV97035.
16.
Senecal S, Victor V, Choudat D, Hornez-Davin S, Conso F. Semicircular lipoatrophy:
18 cases in the same company. Contact Dermatitis 2000; 42: 101-120.
17.
Gruber PC, Fuller LC. Lipoatrophy semicircularis induced by trauma. Clin. Exper.
Dermatol. 2001; 26: 269-271.
18.
Schnitzler L, Verret J.-L, Titon J.-P. La lipoatrophie semi-circulaire des cuisses.
Ann. Dermatol. Venereol. 1980; 107: 421-426.
19.
Pibouin M, Laudren A, Mignard MH, Chevrant-Breton J. Lipoatrophie semi-circulaire
des cuisses. Sem. Hop. Paris 1986 ; 62 : 3760-3762.
20.
Filona G, Bugatti L, Nicolini M, Ciattaglia G; Lipoatrofia semicircolare: due
casi. Unita Operativa di Dermatologia Ospedale " A. Murri" ASL
21.
Dahl PR, Zalla MJ, Winkelmann RK. Localized involutional lipoatrophy: a clinicopathologic
study of 16 patients. J. Am. Acad. Dermatol. 1996; 35: 523-528.
22.
Zalla MJ, Winkelmann RK, Gluck OS. Involutional lipoatrophy: macrophage-related
involution of fat lobules. Dermatology 1995; 191: 149-153.
23.
Petruschke Th, Hauner H. Tumor necrosis factor-a prevents the differentiation
of human adipocyte precursor cells and causes delipidation of newly developed
fat cells. J. Clin. Endocrinol. Metabolism 1993 ; 76 : 742-747.
24.
Prins JB, Niesler CU, Winterford CM, Bright NA, Siddle K, O'Rahilly S, Walker
NI, Cameron DP. Tumor necrosis factor-a induces apoptosis of human adipose cells.
Diabetes 1997; 46: 1939-1944.
25.
Gamaley I, Augsten K, Berg H. Electrostimulation of macrophage NADPH oxidase by
modulated high-frequency electromagnetic fields. Bioelectrochem. Bioenerget. 1995;
38: 415-418.
26.
Maes A,.Verschaeve L. Contractverslag L 3211 2000/TOX/R/002 VITO Boeretang 200
B-2400 Mol
27.
Maes A, Curvers B, Verschaeve L. Lipoatrophia semicircularis: the electromagnetic
hypothesis. Electromagnetic Biology and Medicine 2003; 22 (2), in press.
